
There are several types of Doppler and we will look at all of them. Doppler technology has advanced leaps and bounds in the last two decades. People often ask us why Doppler is always capitalized. This technology is named after Christian Doppler from Vienna, Austria. He discovered the relationship of sound change based on a stationary observer in 1842. Then he developed the formula with a constant. Fast forward over a hundred years and we use several forms of Doppler in every patient exam we perform.
The first application of Doppler was continuous wave (CW) Doppler. These probes have only two crystals; one for sending and one for receiving. It is aptly named because the two crystals are always sending and receiving the signals back from the vessels or chambers. This was primarily used in echocardiography. There is no picture to guide you, only the Doppler waveform on the screen. Therefore the user had to be very proficient in angulation between the ribs. Understanding the way the heart is positioned in the chest and an idea of how the jets flow in the heart is critical in CW. There was no way to improve the image other than using your angles. The most important thing to remember is that the sample line is just that. It returns signals along the entire length of the line that you are aiming into the body. So if you have a chest wall AVM and you are aiming for the mitral valve you will have some very abnormal waveforms with a great deal of superimposition of waveforms.
Now how did the ultrasound industry fix the problems with this type of CW? The manufacturers developed probes in the 1980’s that had what is known as directed CW. This means that even though you have the two crystals continuously sending and receiving you have a picture to guide you. You also have an angle correct available to fine tune the angle parallel to the jet you are sampling. There is also a vast variability of adjustment in the scale and capability to move the baseline. The other theoretical benefit of CW is that there is an infinite scale level. There is only the limitation of the machine to display it. The machine is what caps the scale level. For many years this was only available on phased array probes. This is great for echocardiography but what about the rest of the body?

Picture of a dedicated CW Vingmed probe. Also known as a pencil probe.
When we talk about the scale issue we needed to have a way to increase the scale without CW in a phased array probe. So the manufacturers came up with High PRF. It is the best compromise between Pulsed wave and Continuous wave. This uses pulsed wave so that the technology can be scanned in other types of probes for other body parts. Additional sample volumes are added to the line of the pulsed wave. Due to these other sample volumes you have to make sure that none of these other sample volumes end up in any other vascular structures because the resulting waveform will average all the sample volumes into one waveform that will be very shaggy. Positioning is critical in this instance. Some machines have a button that says HPRF or HiPRF to tell you that you need to push that to obtain a higher scale.
Pulsed wave (PW) is the standard for the majority of exams sonographers perform today. PW is formed by a multichannel system with probes that have several crystals that send and receive in pulses. This form of Doppler has a little box on a line called a sample gate, sample volume or a reference box. You can change the size of the sample gate and slide it up and down along the line. The box will have and angulation bar attached and it varies with the adjustments you make on the user interface. This may be a knob, toggle or switch. The key thing with Doppler is the closer the angle of insonation is to zero the more accurate the waveforms and resulting measurements will be. Any angle over 60 will be inaccurate. Most machines today will show the angle in red if it is over 60 degrees. If your angle is still an issue then you need to reposition your probe, your hand or the patient to meet the 60 degree requirement.
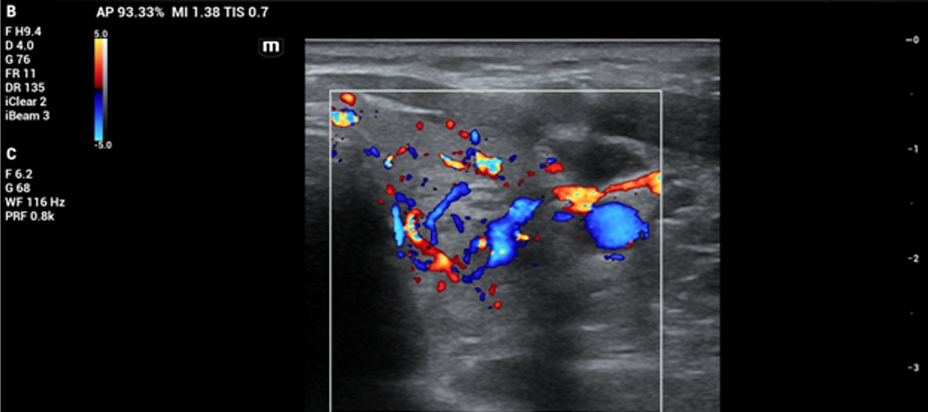
Color flow Doppler is a fast visual that gives a great deal of information in seconds. Colors tell you direction and the scale tells you the relative speed. Blue means that the flow is away from the probe. Red means that the flow is toward the probe. Mosaic means turbulent flow like a stenosis. Color flow is also dependent on angles to have the vessel or the chamber fill in correctly. A multichannel system and a probe that has many crystals are necessary for this to appear in real time. This solved the problem of having to sample in many areas in a vessel, valve or chamber to determine any clinical significance and record it. With color flow you can place the PW sample gate in the area of turbulence or color change and look at the PW waveforms in that area. Then you can apply measurements to the PW waveform to obtain numbers to apply to clinical standards. This speeds up the exam time tremendously.
The last type of Doppler is Power Doppler, Power Angio, Angio, ultrasound angio or amplitude mapping. Angio is short for angiography which is a contrast study used with x-rays. Manufacturers have their own terms for this technology. The correct general term is Power Doppler. This has many of the same characteristic of color flow Doppler but this does not show flow direction. The color maps are also different so there is no confusion about which mode you are imaging a structure in.
This technology is based on the amplitude of the density of the blood cells in a given vessel. The darker the color there is an increased concentration of cells. The lighter the color means a lesser concentration of cells. Some color maps will designate different colors for different amplitudes. Power Doppler is still dependent on the basic quality of the 2D images and the density of the tissues it must pass through. Power Doppler is now used in applications where color flow may be inadequate like tumors. It is used for areas that have low flow and to show where there is inflammation. It is a very sensitive flow detection device.
There are many settings that will improve the visualization of all modes of Doppler. That is beyond the scope of this blog. B-mode imaging is not covered here because it is not Doppler. Doppler is an essential part of all ultrasound exams being performed today.
Please call us with any questions 843-566-1020.
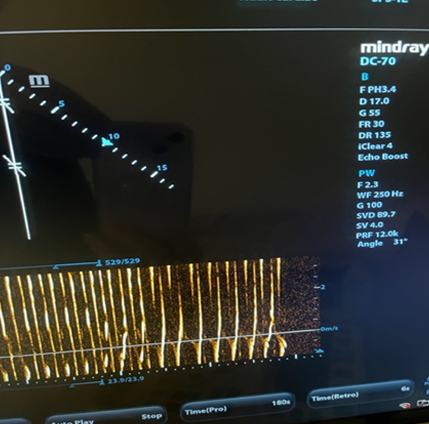
There are two sample volumes (2 curved arrows). Note the up arrow showing the angle correction at 31 degrees.
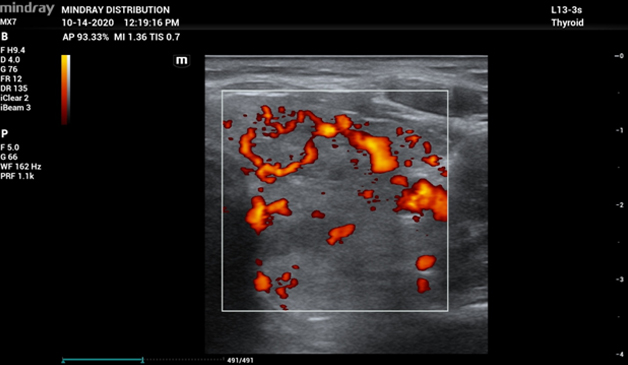
Power Doppler of the same thyroid mass. This is showing better delineation of the blood flow around the mass.